|
|
|
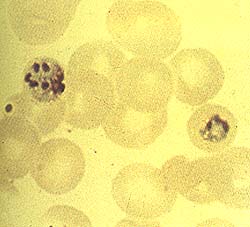
Malaria is the world's leading killer among infectious diseases in tropical Africa, South East Asia, parts of India, Southern China, Latin America, Haiti and some Pacific Islands. It is a parasitic infection acquired when a mosquito injects the parasite into the blood. After a few weeks to several months, those who are infected develop flu-like symptoms, such as high fever, headaches, muscle aches, nausea and abdominal discomfort. If left untreated, the malaria can progress to anemia, heart or kidney failure, coma and even death. Malaria kills more than 1.5 million people each year - approximately one death every 20 seconds. It is firmly rooted in 103 countries, and more than 10,000 American travelers fall ill to it annually. A traveler's best defense against this disease is to take antimalarial drugs and avoid being bitten by mosquitos. They should remain in well-screened areas from dusk to dawn, sleep under mosquito netting, wear pants and long sleeved shirts, and apply mosquito repellent containing DEET to their clothing and exposed skin. In the U.S., doctors prescribe Lariam in travelers' clinics across the country. The drug was debated in medical circles prior to its approval by the U.S. Food and Drug Administration in 1986 because of its reputation for causing adverse effects on the central nervous system.Today, Lariam is the most widely used antimalarial drug in the world. "Over half the patients given high doses of Lariam complained of nausea, dizziness, and fatigue," wrote N.J. White in a study published in the British Medical Journal in January 1994. Lariam is produced in Switzerland by Roche Laboratories. Roche acknowledges its uncertainty about Lariam in their fact-sheet, which accompanies each prescription. "Its exact mechanism of action is unknown," it reads, along with "If signs of unexplained anxiety, depression, restlessness or confusion are noticed...the drug must be discontinued."
Although Lariam is believed to be effective in protecting against malaria, its long term safety in humans is unknown. It should not be taken by patients with a history of epilepsy or psychological disorders, or by people on anti-seizure or heart medication. Lariam should also be avoided by airline pilots and other operators of machinery as it can cause feelings of dizziness, vertigo and confusion. Researcher Christophe Hennequine reported two case studies in the respected journal Archives of Internal Medicine of men who suffered severe side effects from taking Lariam. One healthy 23-year-old man took the standard preventative dose (250 mg) weekly during his trip to the Ivory Coast. After the second dose he acquired intense insomnia and became progressively anxious with feelings of persecution and hypochondria. Three days after his subsequent return from Africa, the man was arrested for aggressive behavior in public. He suffered from memory loss and confusion. Hennequine's second case study was of a 45-year-old Frenchman, also with no medical contraindications, who took Lariam during a visit to Thailand. While there, he developed insomnia, and two weeks later he became melancholic and unable to concentrate. He then deteriorated into serious depression with suicidal impulses.
"Case reports have documented possible Lariam-associated neuropsychiatric reactions, and such reports have lead to a hesitancy among military in the USA to use weekly Lariam as the preferred prophylaxis," added J. L. Sanchez in the prestigious journal,The Lancet. Lariam's effects include "acute brain syndrome," consisting of disorientation and mental dysfunction, and "psychiatric symptoms", such as acute psychosis, memory loss, confusion, hallucinations and behavioral abnormalities -- aggression, agitation, and hyperactivity. Although most of these psychiatric symptoms generally do not last more than 10 days after terminating use of Lariam, severe depression can persist up to nine months. "There is no explanation for these reactions," noted Hennequine.
Despite these findings, the CDC noted in a report posted on the World Wide Web in April 1995, that "minor side effects one may experience while taking Lariam include gastrointestinal disturbances and dizziness, which tend to be mild and temporary. More serious side effects at the recommended doses have rarely occurred." The World Health Organization currently recommends either Chloroquine / Paludrine or Lariam - but explicitly states no order of preference. The CDC favors Lariam, and the FDA has not approved Paludrine for sale in the United States. In the United Kingdom, two medical research laboratories, Malaria Reference Laboratory and Ross Institute, recommend Chloroquine / Paludrine - with Lariam to be used only as an option for short term travel in areas of highly resistant malaria, notes researcher Robert Steffen in The Lancet in May 1993. Travelers may find a safe and effective alternative in the Paludrine / Chloroquine combination, which can be purchased over-the-counter in any almost any pharmacy outside the United States. "In the prophylaxis of malaria, Chloroquine / Paludrine has an excellent safety record, being rarely associated with severe adverse reactions in the recommended doses," wrote G.A. Luzzi in the medical journal Drug Safety. The rate of severe reactions is less than one in 100,000. Reported side effects include mouth ulcers and temporary hair loss.
Although most effective when combined with a weekly dose of Chloroquine, Paludrine, which has been used in Europe since 1948, is a highly effective and safe antimalarial drug that can be used alone against the chloroquine-resistant P. falciparum malaria, notes researcher C.G. Nevill in The Transactions of Royal Society of Tropical Medicine and Hygiene. Unlike Lariam, Paludrine is safe in breast feeding and pregnant women. "Paludrine has been widely used for over 40 years and ... most people take it without any problems," noted Paludrine's manufacturer, Zeneca Corp., in their drug sheet. The risk of malaria is dependent upon the duration of a traveler's stay in rural areas and the type of malaria present. When prescribing antimalarials, physicians must consider that the drugs are being given to healthy people to keep them from becoming sick. "Therefore, a careful assessment is required to ensure that the risk of toxicity of the antimalarial drug does not outweigh the risk of acquiring malaria," noted Luzzi. "I couldn't tolerate it," said Artie Jenkins, who took Lariam during a 10 day safari in Kenya, East Africa, in 1992. "It gave me terrible heartburn and gastrointestinal problems, so I just stopped taking it. I thought I'd rather get malaria than deal with taking Lariam."
Recognizing the limitations of antimalarial drugs and the complexity of the malaria situation worldwide, the World Health Organization recommends that in addition to, or sometimes instead, of antimalarial drugs, travelers should carry with them a treatment medication for emergency uses when malaria is suspected and medical help is unavailable. As research continues, scientists will undoubtably learn more about both Lariam and Paludrine / Chloroquine. But the next time I visit East
Africa, I will plan a stop-over in England to purchase a supply of Paludrine / Chloroquine
first. Links:Updated information at: National Center for Biotechnology Information References:
|
| |||||||||||

 awoke suddenly from a terrible nightmare with sweat beading down my
forehead. My sleep was haunted by terrifying visions and my days were plagued by anxiety
and restlessness. I thought I was suffering a nervous breakdown in the middle of Tanzania,
East Africa.
awoke suddenly from a terrible nightmare with sweat beading down my
forehead. My sleep was haunted by terrifying visions and my days were plagued by anxiety
and restlessness. I thought I was suffering a nervous breakdown in the middle of Tanzania,
East Africa.